 1-800-834-3059
1-800-834-3059
By AccentCare
 Have you ever been minding your own business when you were interrupted by pesky hiccups? One minute you are having a conversation with a friend and then all of sudden -- “HICCUP!” -- you are interrupted by the sudden intake of air! Most of us have experienced this at least a few times in our lives. While for many these episodes are trivial and even embarrassing, for some hiccups can be more serious, chronic, and might denote an underlying condition which needs treatment. Let’s take a look at a case.
Have you ever been minding your own business when you were interrupted by pesky hiccups? One minute you are having a conversation with a friend and then all of sudden -- “HICCUP!” -- you are interrupted by the sudden intake of air! Most of us have experienced this at least a few times in our lives. While for many these episodes are trivial and even embarrassing, for some hiccups can be more serious, chronic, and might denote an underlying condition which needs treatment. Let’s take a look at a case.
Ron, is a 79 year old man admitted to hospice with a diagnosis of end-stage esophageal cancer and wide-spread metastasis. He tells his hospice nurse that he has had persistent hiccups for 4 days now. He exclaims “It’s bad enough that I’ve been hiccuping so long that my abdominal muscles now hurt, but the pain in my ribs where the cancer has spread is off the chart when I hiccup. I try to not breath because every time I hiccup it’s like getting kicked in the ribs. This has to stop.” Poor Rom, we can all imagine how distressing this can be. Let’s do a bit of a deeper dive.
Why do hiccups occur?
Ron, like most people, has had hiccups before but really never thought about why they happened. Ron’s nurse explained that a hiccup, or singultus as it is medically termed, is caused by an improper reflex or spasm of the muscles used to take in breath.1 During this phenomenon the glottis, a flap that protects the airway while we eat by closing off the airway, slams shut right after the start of inspiration. This premature closing of the airway causes the sound and maneuver that we know as a hiccup.1
What are some of the clinical features of hiccups?
Ron asks his hospice nurse what causes hiccups. A little research shows that the most common cause of hiccup is gastric reflux and distention. Peripheral causes of hiccups can be divided into gastrointestinal and non-gastrointestinal. Gastroesophageal reflux disease (GERD), hernia, malignancy, gastroparesis, and peptic ulcer disease are examples of gastrointestinal conditions that can results in hiccups. There are MANY non-gastrointestinal causes of hiccups such as aortic aneurysm, bronchitis, pneumonia, asthma, myocardial infarction, pericarditis, tuberculosis, rhinitis, otitis, pharyngitis and more! Hiccups may also be caused by electrolyte imbalances, medications, alcohol, diabetes, anxiety, and stress.2 Ron obviously has a malignancy and he’s long been a GERD-sufferer. Many of the causes of persistent, intractable hiccups are a result of underlying conditions as described in the table but many have to do with the irritation of the vagus or phrenic nerve to cause the abnormal spasm of the two reflexes. Something as rare as hair pressing against the tympanic membrane of the external ear canal can cause hiccups and taking it out can remedy the situation.
The harmless, fleeting hiccups that many experience as children and sometimes as adults are called “benign, self-limiting” and are defined as lasting less than 24 hours.1 Hiccups lasting more than 48 hours are considered “persistent” after 48 hours, and intractable if persisting more than a 1 month.3
What are some of the nonpharmacologic treatment options for hiccups?
Nonpharmacologic treatment of hiccups is widely debated and is somewhat learned from experience. The theory behind these strategies is if you stimulate the pharynx by various means then the vagal nerve portion of the reflex causing the hiccups will be blocked and the hiccups will stopped.1 Below are a few options for non-pharmacologic treatment for hiccups.
Physical maneuvers:1
- Remove foreign body from ear
- Swallow a teaspoon of sugar
- Sip ice water
- Drink water quickly
Interrupt respiratory cycle:1
- Breath holding
- Sneezing
- Gasping
- Rebreathing into a bag
- Valsalva maneuver (breathing out of the mouth with nose clamped shut)
Ron told the doctors that for the last 3 days he had tried it all. His wife tried to scare him (Mrs. Ron that was risky business!), he tried to hold his breath, and took a teaspoonful of sugar but nothing worked. Many other physical maneuvers were tried but none relieved the hiccups. Upon examination of the ear canal, the doctor finds a hair pushing up against the tympanic membrane. After removal, the hiccups are still persistent. At this point, pharmacologic options are considered for Ron.
What are the pharmacologic treatment options for hiccups?
When possible, the treatment of hiccups should target the underlying cause. Many medications have been used to treat chronic hiccups including chlorpromazine (Thorazine), haloperidol (Haldol), benzodiazepines (e.g., lorazepam [Ativan]), gabapentin (Neurontin), metoclopramide (Reglan) and baclofen (Lioresal).2 Generally speaking, these medications act by either the dopaminergic or GABAergic pathways.2 While chlorpromazine has been used for many years for this indication, the significant side effects, and better data associated with other medications has rendered chlorpromazine less useful.
When hiccups are due to GERD or some other gastrointestinal cause, a proton pump inhibitor (PPI; e.g., omeprazole) or metoclopramide (Reglan) may be helpful. The PPIs may act by lowering acid secretion.2
Jeon and colleagues propose the following strategy in the management of hiccups in a patient with a serious, advanced illness:
- A hospice or palliative care patient with persistent hiccups causing distress and non-pharmacologic interventions have not been helpful:
- If the patient is in the last few days of life, consider parenteral midazolam (Versed)
- Try to identify any reversible causes and act according
- If this is not beneficial, consider a PPI (e.g., omeprazole)
- If these interventions are not successful, for peripheral gastrointestinal causes of hiccups consider:
- Metoclopramide (Reglan) or PPI first line
- Baclofen (Lioresal) or gabapentin (Neurontin) second line
- Alternatives: chlorpromazine, midazolam, nimodipine, olanzapine, lidocaine, or methylphenidate
- For non-gastrointestinal causes of hiccups consider:
- Metoclopramide first line
- Same second line and alternative agents as gastrointestinal causes
- Centrally-mediated hiccups
- Consider baclofen (Lioresal) as first line
- Gabapentin (Neurontin) as second line
- Alternatives: haloperidol (Haldol) or nimodipine (Nymalize)
- If all this fails, consider a procedural intervention (phrenic or vagal nerve blockage or stimulation)
A summary of dosing of these medications is as follows:2
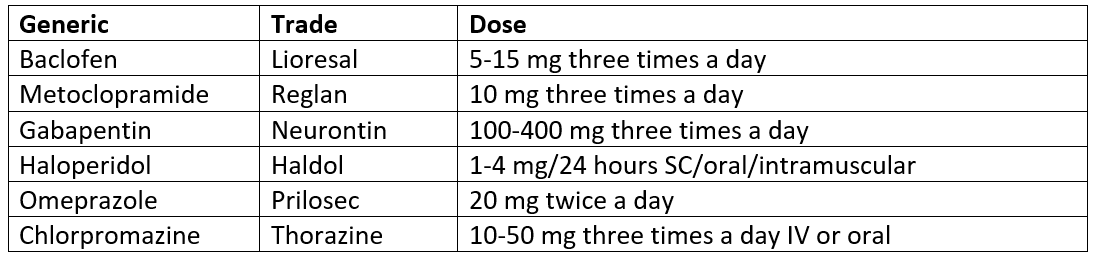
Ron is started on the PPI omeprazole to treat the underlying condition of GERD and metoclopramide to treat the hiccups. Upon follow up, Ron’s hiccups are under control. Ron was greatly relieved about the hiccups resolution.
Hiccups are a trivial phenomenon for most individuals usually in childhood and sometimes into adulthood but can cause severe discomfort if persistent for a long period of time. They usually are a sign of an underlying condition which should be treated first before other pharmacological options are considered. So next time your conversation is interrupted by a bout of hiccups you can think about this issue of PharmSmart!
References:
- Stapczynski J. Respiratory Distress. In: Tintinalli E, MA O, Yealy DM, et al., eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 9e. McGraw-Hill; Accessed July 1, 2020.
- Jeon YS, Kearney AM, Baker PG. Management of hiccups in palliative care patients. GMJ Supportive & Palliative Care 2018;8:1-6.
- Woelk CJ. Managing hiccups. Can Fam Physician. 2011;57(6):672-675.
- In: Papadakis MA, McPhee SJ, Bernstein J, eds. Quick Medical Diagnosis & Treatment 2020. McGraw-Hill; Accessed July 1, 2020.
PharmSmart is a monthly article dedicated to best practices in drug management for patients nearing the end of life, with a little cheer and lightheartedness woven throughout. It is edited by Dr. Mary Lynn McPherson, PharmD. Dr. McPherson is the Executive Director of Advanced Post-Graduate Education in Palliative Care at University of Maryland. Dr. McPherson is a consultant pharmacist to Seasons, and answers complex medication questions for our clinical teams at all hours of the day or night. She is a nationally-recognized expert in medication management for hospice and palliative care patients.